
Fact Check: "All Fired Up" on Semaglutide and Cardiovascular Health

This isn’t about Maintenance Phase, but misinformation about semaglutide and the drug industry is rampant, and this is a prime example. Up front, I want to acknowledge that there are good reasons to have negative feelings about large pharmaceutical companies - there are numerous examples of pharma companies acting unethically and valuing profit above patient lives. However, there are far more examples of pharma companies acting ethically and developing lifesaving or life-changing medications. Think of how many drugs exist! According to the FDA, there are over 20,000 prescription drug products on the market. And that’s just the prescription ones! I don’t say that to minimize the horrifying actions of Purdue in the opioid crisis or GSK’s criminal actions regarding Wellbutrin, Paxil, and Avendia, etc., but we do need to recognize that not everything a pharma company does is nefarious. As is true of any industry, there are things that outsiders may view skeptically that those of us with more inside experience understand as reasonable and/or necessary. There are some people on the internet who are weaponizing the general public’s lack of knowledge about the pharmaceutical industry to make it seem like Novo Nordisk is doing outlandish appalling things like faking data or rigging their studies. I am not here to defend Novo Nordisk as a company or to say that their actions with semaglutide or any of their other products have been 100% above board. But I think it is important to counter these dangerous narratives that are popping up that suggest that things that are completely normal and reasonable are signs of evil Big Pharma trying to hoodwink us. In a time of so much misinformation, we need to be skeptical of anyone without actual expertise in an area telling us they are the one you should listen to on a topic. As is evidenced in this podcast episode, neither the host nor the guest have a solid grasp on statistics, nor does either of them understand the ins and outs of designing and conducting clinical trials. This podcast is a really great example of the gish gallop debate tactic, “drowning your opponent in a flood of individually weak arguments in order to prevent rebuttal of the whole argument collection without great effort.” The host and the guest frequently throw out statements that contradict each other or make no sense, like saying the Independent Data Monitoring Committee was biased and then proceeding to say that the Independent Data Committee guidance was in opposition to the desires of the Novo Nordisk shareholders.
I need to state here that the issue is never with the messaging that body fat is not an indicator of health or the value of a human being; the issue is with underqualified and undereducated individuals misunderstanding and misrepresenting research and biology. We’re witnessing the real time development of a misinformation ecosystem along the same lines of the Rogan-Huberman axis, just around health research rather than vaccines or sunscreen or longevity. There are already examples of these podcasts referencing each other and recommending that listeners “learn more” by listening to an episode of Maintenance Phase. These individuals are clearly not familiar with industry practices and are misinterpreting completely normal and valid practices as nefarious, or outright fabricating issues that do not exist.
I decided to do this fact-check in a slightly different format for a couple of reasons. First, I’ve definitely heard the feedback that the MP fact-checks are long and dry. Second, there is a lot of repetition of the same misinformation in this episode. So I decided it made more sense to write up the claims made in the podcast and what is wrong about them, instead of a line-by-line assessment. I’ve linked to a relevant quote from the transcript for each claim. Here are the claims that I address:
The press release and the 20% reduction in cardiovascular events are a “straight up lie.”
Semaglutide doesn’t work.
The results of the SELECT trial are questionable because it’s a “conflict of interest palooza.”
Novo Nordisk is “hoarding the data”.
Novo Nordisk paid the statisticians.
SDTM is an “interpretation of raw data”, and the data are whitewashed.
Novo Nordisk didn’t test lower doses of semaglutide.
It’s a problem that these patients are from all over the world, with only a few at some sites, because no one can see the “big picture” except for Novo Nordisk.
Novo Nordisk intentionally made the trial population mostly White and mostly male.
The 27 kg/m^2 BMI cutoff for inclusion is “weird.”
Novo Nordisk “stacked the deck” by including people with established cardiovascular disease.
It’s “ghoulish” that Novo Nordisk waited around for people to have cardiovascular events.
Clinical trials sometimes “run the data continuously” until they “hit a point where they have a statistically significant outcome.”
The Independent Data Monitoring Committee is fraudulent because all of the members have been paid by Novo Nordisk.
The CEO of Novo Nordisk previously said the trial needed to result in an 80% reduction for the drug to be viable.
The reduction in risk was 1.5%, not 20%.
Novo Nordisk picked just 3 of the Major Adverse Cardiac Events (MACE) and the outcome is a “mash up of the things that can go wrong, heart wise, because it takes too long for and it’s too expensive” for researchers to assess heart attack vs stroke.
Novo Nordisk couldn’t “confidently analyze” whether or not semaglutide reduced heart attack or stroke, specifically or whether or not the weight loss was related.
It is odd that Novo Nordisk published a paper about 4 year weight-loss among participants in a cardiovascular health trial when they had a weight loss trial.
Statins are more effective at reducing cardiovascular risk than semaglutide.
The FDA approved semaglutide for adults with “overweight and obesity”, but “that wasn’t really who that this trial was for.”
After 2 years, only 25% of people are still taking semaglutide.
“A significant number of people got up to 2.4 but then titrated right back down again.”
Intentional weight loss leads to earlier mortality in adults over 65.
The host says, “I haven’t seen any research they’ve provided to suggest any better outcomes for people on this drug.”
Australia has “resisted” Novo Nordisk’s “attacks” because the Pharmaceutical Benefits Advisory Council told them it would be too expensive and “you haven’t provided us any information on whether or not this will improve health beyond just the weight loss stuff.”
Russia has approved “bootleg versions of Ozempic to be sold.”
Novo Nordisk attempted to cover up the analysis about CVD risk and weight loss because the results were not what they wanted.
Claim: The press release and the 20% reduction in cardiovascular events are a “straight up lie.”
Fact: It is very common for pharmaceutical companies to issue press releases prior to the study being published. The claim that there is no study and no actual research to back this claim is a misunderstanding of how pharmaceutical development works. There is indeed a study: the clinical trial that is mentioned in the press release. The data from that trial have been analyzed and revealed a 20% decrease in cardiovascular events. This does not mean that the whole study is ready to be published as a manuscript – the manuscript writing and publishing process is very long. There are many rounds of both internal and external (i.e., peer) review. And this is not unique to Novo Nordisk or semaglutide - you can look online and find tons of press releases about drugs without full manuscripts accompanying them. It’s not about “bothering to release them at the same time”, it’s that the timelines for these things are totally different. The 20% figure isn’t a “claim” that needs to be questioned, as the podcast implies – it’s a readout of the data from the trial.
The host also says that the press release is misleading because the headline says there’s a 20% risk reduction in adults with “overweight or obesity” when, “in fact, it’s over 45 with existing cardiovascular disease, without type two diabetes and a BMI over 27.” In the press release, the sentence about the 20% reduction is directly preceded by a sentence that says, “The trial enrolled 17,604 adults aged 45 years or older with overweight or obesity and established cardiovascular disease (CVD) with no prior history of diabetes. The trial achieved its primary objective by demonstrating a statistically significant and superior reduction in MACE of 20% for people treated with semaglutide 2.4 mg compared to placebo.”
TLDR; It is not expected that manuscripts accompany press releases, and the press release contains an accurate description of the trial data. The headline might leave out the ‘without diabetes and with CVD’ but that information is stated in the first paragraph.
Claim: Semaglutide doesn’t work.
Fact: I’m not exactly sure that I need to correct this one, as it seems obvious that it is incorrect. I don’t know what the host means by “work” here, but if you really need to be convinced, here is a systematic literature review and meta-analysis of the efficacy of semaglutide for type 2 diabetes, and here is a systematic literature review and meta-analysis of the efficacy of semaglutide for weight loss among individuals without type 2 diabetes (and here is another!).
Claim: The results of the SELECT trial are questionable because it’s a “conflict of interest palooza.”
Fact: This is not unique to semaglutide or Novo Nordisk. Every pharmaceutical company pays consulting fees to clinicians. They get those fees whether or not the drug works well, and they don’t get dividends for drug sales. So I’m not sure why this is a concern here, nor what a viable alternative would be.
Claim: Novo Nordisk is “hoarding the data”.
Fact: Novo Nordisk did not agree to share the data from the SELECT trial. This is very common. A 2016 study found that only 25% of large randomized cardiovascular health clinical trials (>5000 patients) from top 20 pharma companies (based on 2014 global sales figures) made their data available for sharing. Another study in JAMA Network Open from 2021 found that while 68.6% of the 487 clinical trials published in 2018-2020 in JAMA, Lancet, and New England Journal of Medicine reported data sharing, only 2 (0.6%) trials actually made their data available on the journal website. And while 89 studies reported the data would be stored in a secure repository, data were available for only 17 of those studies. The point is data sharing is rare. Is not sharing data ideal? No. But it’s common and not unique to this company.
Claim: Novo Nordisk paid the statisticians.
Fact: My takeaway here is that because the statisticians are paid by their employer, they are not to be trusted. I’m not sure if the host expects that individuals work for free, but I think we can all agree that it makes sense that Novo Nordisk pays their statisticians and I’m not sure what the alternative would be. I don’t think I need to point out that this is how all studies work and is not unique to Novo Nordisk or semaglutide, but I’ll put that out there just to be safe.
Claim: SDTM is an “interpretation of raw data” and the data are whitewashed.
Fact: The Study Data Tabulation Model (SDTM) is a standard for formatting and organizing clinical data that is required for submissions to the FDA and PMDA (Japan). It makes data review and the regulatory process easier because it allows for replication and traceability of analysis. In other words, this is a standard put in place to make things more transparent. SDTM is not an “interpretation” of the data, nor is providing SDTM data to the external statisticians a form of “whitewashing.” A great website to visit if you want to learn more about SDTM is the Clinical Data Interchange Standards Consortium “Standards” page. You can also learn more about FDA data standards on their website.
Claim: Novo Nordisk didn’t test lower doses of semaglutide.
Fact: The STEP 2 trial compared 1.0mg semaglutide to 2.4mg and found that 2.4mg led to greater weight loss while tolerability (i.e., adverse events) were similar across doses. That is how 2.4mg was chosen as the dose. It would not make sense to test a different dose for cardiovascular outcomes if 2.4mg is the clinical dose.
Claim: It’s a problem that these patients are from all over the world, with only a few at some sites, because no one can see the “big picture” except for Novo Nordisk.
Fact: This is common for large trials. It is actually better to have patients from many different places and clinics, both for the sake of diversity and because it means that there is less risk of bias due to differences in clinical care at a single site. The sponsor (i.e., pharma company) and/or an independent review committee are always the only ones who can “see” all the data during the trial. That is a matter of data privacy and integrity. The study Appendix explicitly states that all of the authors had access to the analyzed datasets. That being said, Novo Nordisk was not looking at the data continually throughout the trial. See my comment about “running the data continuously” below.
Claim: Novo Nordisk intentionally made the trial population mostly White and mostly male.
Fact: I’ve addressed this before in some of the MP episode fact-checks, but it is a very well-known issue that clinical trials lack diversity. Novo Nordisk is not alone in this. That doesn’t mean it is acceptable - it’s just not Novo Nordisk’s fault nor is it part of some semaglutide conspiracy that SELECT was mostly White and mostly male. As for the sex imbalance, it actually makes quite a bit of sense. In order to participate in SELECT, you could not have already taken semaglutide. We know (as does the host because she mentions this in the podcast) that the weight-loss trials for semaglutide were majority female (STEP 3 was 81% female, STEP 5 was 77.6% female). So, who is left to participate in this trial? Probably a lot more men! There is also evidence that women are underrepresented in cardiovascular drug trials on the whole. Again, not a Novo Nordisk thing.
In fact, the Appendix calls out the lack of diversity explicitly: “The SELECT trial does not duplicate a globally representative population of overweight and obesity complicated by established cardiovascular disease, but it does offer broad representation of some subgroups for analysis… This predominantly White population would be more representative of the global burden of disease if there were more Black and Asian participants to allow more meaningful analyses based on race.” And a recent press release based on the new analyses exploring weight loss in SELECT reads: “Despite these important findings, the authors caution that SELECT is not a primary prevention trial so that the data cannot be extrapolated to all adults with overweight and obesity to prevent MACE; and despite being large and diverse, it does not include enough individuals from different racial groups to understand different potential effects.”
Claim: The 27 kg/m^2 BMI cutoff for inclusion is “weird.”
Fact: All of the STEP trials used a cutoff of 30 kg/m^2 or 27 kg/m^2 with at least one comorbidity. This isn’t weird, it’s consistent. There is also recent research that suggests that 27 kg/m^2 should be the new cutoff for “obese” in middle aged and older adults. I’m not supporting this change, nor do I think BMI is necessarily an indicator of health. I’m just explaining that this is not “weird” and if the host and guest had read up on all the relevant research, they might not think it was weird, either.
Claim: Novo Nordisk “stacked the deck” by including people with established cardiovascular disease.
Fact: I think this is just a misunderstanding of the study. Novo Nordisk was quite explicit that the objective of SELECT was to “explore the superiority of a long-acting, weekly GLP-1 RA (semaglutide 2.4 mg) versus placebo for reduction of cardiovascular events in patients with established CVD and overweight or obesity but without established type 2 diabetes.” It’s not stacking the deck to require that your study population has CVD when your objective is to investigate the effect of your drug in patients with CVD.
Claim: It’s “ghoulish” that Novo Nordisk waited around for people to have cardiovascular events.
Fact: This is how randomized placebo-controlled trials work and it comes down to a very serious ethical concept in clinical trials that is called “equipoise.” Clinical equipoise refers to genuine uncertainty about which treatment option is better. This is why certain things cannot be studied in randomized placebo-controlled trials. For example, this is why the evidence linking smoking to lung cancer did not come from randomized trials. It would have been unethical to do a randomized trial to assess smoking and lung cancer (i.e., randomize some people to smoke cigarettes and others to abstain and then see if the risk of lung cancer differs between the two groups), because there was already substantial evidence from population-based studies that smoking was dangerous. In the case of the SELECT trial, researchers and clinicians did not know if semaglutide reduced the risk of cardiovascular events. Therefore, it was ethical to conduct the study. Importantly, they incorporated a “stopping rule” into their study so that if a protective effect was seen early on, the trial could be stopped, allowing patients in the placebo arm to receive semaglutide. (See my comment about “running the data continuously” below.)
As an aside, if the host truly believes that semaglutide doesn’t have any protective effects, this is a confusing issue to raise.
Claim: Clinical trials sometimes “run the data continuously” until they “hit a point where they have a statistically significant outcome.”
Fact: This is an outrageous claim that is also later contradicted by the host, who proceeds to say that Novo Nordisk called the trial early. Clinical trials are highly regulated and planned down to the tiniest detail. What the host is implying here absolutely does not happen. The stopping criteria for a trial are defined a priori in the protocol. There are a variety of reasons that we can’t say exactly how long a trial will take. First, recruitment timelines are unpredictable. The SELECT trial, for example, estimated 28 months for recruitment. From my experience, plenty of trials take longer to recruit and enroll patients than originally anticipated. This means that the study will last longer from study open to last patient follow-up. Additionally, in a trial like SELECT, where the outcome is what we call “time-to-event”, the duration of the trial depends on how many patients have events and the timing of those events. This is explained thoroughly in the SELECT study methods:
“This event-driven trial was designed to provide 90% power to detect a relative risk reduction of 17% for a primary end-point event in the semaglutide group as compared with the placebo group (hazard ratio, 0.83) at an overall one-sided significance level of 0.025. This design required that a minimum of 1225 primary end-point events be accrued. Assuming an event rate for the primary end point of 2.2% per year in the placebo group, a trial duration of 59 months, and a withdrawal or loss-to-follow-up rate of 1% per year in both groups, we estimated that 17,500 patients would need to be enrolled. One interim analysis for superiority with respect to the primary endpoint was prespecified to occur when two thirds of the total planned number of primary end-point events had accrued (additional details are provided in the Supplementary Appendix).”
The event rate that the sample size calculation is based on is an estimate which means there is some uncertainty. In reality, the number of events that need to occur in order to detect a difference between groups when one truly exists may occur faster or slower than that estimated rate. This impacts the duration of the trial.
This point is related to another claim that the host makes at one point, which is that there is something fishy going on because the CEO said they’d need to find a 20% reduction and then, lo and behold, they did. See the point below about this.
Claim: The Independent Data Monitoring Committee is fraudulent because all of the members have been paid by Novo Nordisk.
Fact: Below are the members of the IDMC. The host first says that all seven members of the IDMC received payments from Novo Nordisk and then subsequently says that all she could see was that three of them did. The three Americans who did receive payments, Mark Schattner, Robert Gagel, and Christopher Granger, all received money from Novo Nordisk for consulting fees and travel and lodging in 2019 and prior and have not received any money from Novo Nordisk since. Per the FDA guidelines, “DMC members should have no ongoing financial relationship with a trial’s commercial sponsor…” Which is true of all of these folks. It also makes quite a lot of sense that these members had previously been consultants for Novo Nordisk, because when selecting members for an IDMC, guidelines suggest choosing people with demonstrated expertise in the field, including trial experience and publications. Since pharma companies pay consulting fees to many clinicians, it is reasonable that experts in the field who are established enough to be selected for an IDMC would have previously been brought on as consultants.
It might help dispel some of the conspiracy here if we think about what the IDMC actually did. Their role here was to look at the unblinded data part way through the trial and to determine if the trial should continue or not. If it did not look like the drug was working, if the evidence was incredibly obvious that the drug was working and therefore it would be unethical or keep patients on placebo, or if the drug was harming patients, they would end the trial early. In fact, Novo Nordisk did just this with their FLOW trial. The IDMC suggested that they terminate the trial early, because the interim analysis showed strong efficacy (again, also the opposite of the aforementioned “running the data” until they get significant results). The host later says that the shareholders wanted to end SELECT early (I don’t know where she got this information), but the company said no due to IDMC guidance. The host is simultaneously saying the IDMC is biased and saying the IDMC acted against the shareholder requests, thereby refuting her own accusation of misconduct.
Claim: The CEO of Novo Nordisk previously said the trial needed to result in an 80% reduction for the drug to be viable.
Fact: I’ll preface this by saying that I can’t find any source for this. But for fun, let’s just say he did say something like this, so we can delve into some more statistical concepts. This might get a bit technical so I’ll add a TLDR at the bottom. Ok, there is a concept in statistics called “power”. You will see this referenced in the methods section from the SELECT manuscript that I quoted above. Statistical power is the ability to detect a statistically significant result when one truly exists. In clinical trials, this is usually set to 80% or 90% and it is directly related to the sample size for the anticipated effect (i.e., magnitude of the hazard ratio in SELECT). If your sample size is too small, your effect estimate (i.e., hazard ratio) may not be statistically significant even if the drug really does work. The smaller the anticipated effect size, the more people you need in your study in order to detect the effect. In other words, large effects are easier to detect. Ok, with that in mind, let’s revisit the supposed statement from Novo Nordisk CEO Lars Jorgensen.
As indicated in the methods section that I included above, the SELECT trial was powered to detect a 17% risk reduction in the primary endpoint. This means that if the true risk reduction was smaller than 17%, the study would be underpowered (i.e., less likely to identify a true effect when it exists). So the study wasn’t rigged - it’s not some big conspiracy. It’s that if the true effect was smaller than a 17% reduction, the results may have been erroneously null.
Claim: The reduction in risk was 1.5%, not 20%.
Fact: It is definitely important to consider the absolute risk difference alongside the relative risk difference. I’ll touch on why both are important in a second. But first, I want to clarify that 1.5% is NOT the absolute risk difference. To explain why this is, we need to look at where the 20% risk difference came from. The analysis in this study is a very common type of analysis that is used for what we call “time-to-event” outcomes (i.e., we are following someone until they have a specific outcome or until the end of the study). The statistical model is called a Cox Proportional Hazards model and the result of the model is what we call a hazard ratio, which for these purposes we can think of as an estimate of the risk in one group relative to the risk in another group (there are nuances to a hazard ratio that make it not equivalent to a risk ratio, but that’s for another day). One of the important elements of a Cox model is that it accounts for what we call “censoring”, which is when something precludes us from observing if a patient has an event (i.e., study period ends, patient is lost to follow-up, patient dies [unless the outcome of interest is mortality, obviously]). So the hazard ratio from SELECT is 0.80, meaning that the “risk” of cardiovascular events is 20% lower in the treatment arm than in the control arm. You’ll notice that if you just divide the percent of patients who had an event in the treatment arm (6.5%) by the percent of patients who had an event in the control arm (8.0%), you get 0.8125, not 0.80. This is because the hazard ratio is taking into account censoring, as I described above. Ok, with that part out of the way, you probably have figured out why simply subtracting 6.5% from 8.0% does not give an accurate absolute risk difference. Those numbers do not reflect censoring. If you wanted to assess the absolute risk difference in a statistically correct way, you’d need to assess the proportion of patients who had events using a method that accounts for censoring, not just use the raw proportions of patients in each arm who had an event. If I had the raw data, I could calculate the absolute risk difference, but without the individual patient data, I can’t. And neither can the guest or the host.
Ok, with that out of the way, I want to say that while the guest in this podcast is implying that the use of a relative risk measure in the reporting of SELECT results is intentionally misleading, if you take some time to look at the literature or results from virtually any clinical trial, you will see that results are almost ALWAYS reported as relative risks, not absolute. So this is not unique to SELECT. That being said, it is very important that people understand the difference between relative and absolute measures of risk, and ideally we would be presented with both (this is an ongoing topic of debate in epidemiology, similar to the debate over p-values). In my opinion, absolute risk differences are most useful when thinking about the potential effect of a drug for you, as an individual. But absolute risk differences are not particularly useful when assessing efficacy, because a 1.5% difference means really different things depending on the baseline rate. For example, say a drug reduces the risk of death from 95% to 93.5%. Would we say that’s an effective drug? The relative reduction is miniscule (<2%). In contrast, if a drug reduces risk from 3% to 1.5%, that’s a 50% reduction! The point is, there is value to both absolute and relative measures of risk, and it’s important to consider both when thinking about the benefits/risks of an intervention.
The guest says, “we’re taught in statistics that if anyone’s using relative risk reduction without telling us more like they’re selling something.” This is not something that they teach in statistics - the guest’s statistical training may have included something like this, but her training is not in advanced statistics. What you ARE taught in statistics is how to think about relative vs absolute risk differences and when each might be most useful. If the prevailing belief was that relative risks were shady, you wouldn’t see them in virtually every peer-reviewed paper that estimates a risk difference, right?
Note that I have now seen the 1.5% figure mentioned in multiple places, including Forbes and Medscape, so the guest here is not the only one to make this mistake.
Claim: Novo Nordisk picked just 3 of the Major Adverse Cardiac Events (MACE) and the outcome is a “mash up of the things that can go wrong, heart wise, because it takes too long for and it’s too expensive” for researchers to assess heart attack vs stroke.
Fact: There is debate in the scientific community about which components to include in the Major Adverse Cardiac Events (MACE) composite endpoint. That being said, the composite endpoint is not used because they are lazy or want to spend less money - it’s because the outcome of interest is “cardiovascular disease” which quite literally encompasses all of those endpoints because they are all sequelae of atherosclerosis. It is therefore relevant to assess all of them together. Also, Novo Nordisk didn’t just pick and choose 3 components of MACE - the 3-point MACE is very commonly used in clinical trials, including prior studies of semaglutide in patients with diabetes (ref 1, ref 2, ref 3). The 3-point MACE is also endorsed by the FDA (ref 4).
It’s also worth noting that if Novo Nordisk had included more components in the composite endpoint, as it seems the guest is implying would be better, the effect size would likely be even larger, because even more events are classified as events of interest.
Claim: Novo Nordisk couldn’t “confidently analyze” whether or not semaglutide reduced heart attack or stroke, specifically or whether or not the weight loss was related.
Fact: First, the primary objective of this study was not to assess if weight loss was the mechanism by which semaglutide reduced risk of cardiovascular events. So that point is irrelevant. This point is repeated multiple times, as if Novo Nordisk is trying to hide the fact that weight loss wasn’t tied to the reduction in cardiovascular risk (though there is an addendum about the recently released results that misinterprets the findings). It’s not a “gotcha” as the host thinks it is - it just wasn’t part of the primary objective of the study. I’m also not sure what the “gotcha” is here - so what if the drug works to reduce cardiovascular risk through a different mechanism than weight loss? Great! That’s awesome! I’m not sure why the host and the guest are so opposed to a drug that improves cardiovascular health. She seems to be ok with statins, so I don’t see how this is any different.
Second, as mentioned above, the study was not intended to disentangle the effect of semaglutide on each of the MACE components. They are all sequelae of atherosclerosis and therefore assessing them as a composite outcome is scientifically sound.
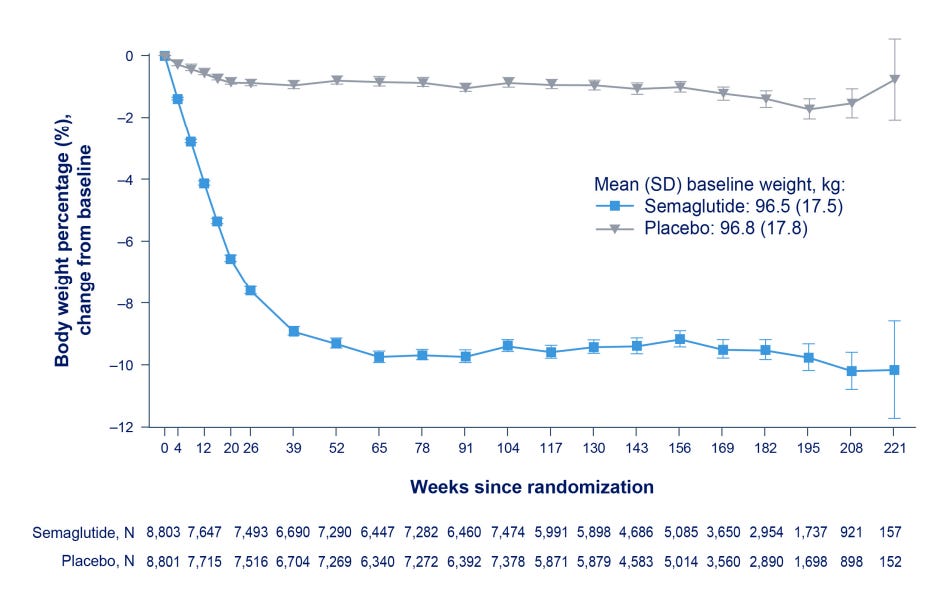
Claim: Only people who continue losing weight continue to come to weigh-ins.
Fact: I agree it’s pretty bad how much attrition there was in the weight data in SELECT, but the attrition occurred equally across arms and the placebo arm had basically no reduction in weight (see graph below from the Appendix, p. 36). So this explanation makes no sense.
Claim: It is odd that Novo Nordisk published a paper about 4 year weight-loss among participants in a cardiovascular health trial when they had a weight loss trial.
Fact: This one seems pretty obvious to me, but just in case it isn’t obvious, the SELECT trial had around 5 years of follow-up. The STEP 5 trial had 2 years of follow-up. You can’t publish data you don’t have. This is also confusing given that the host implies that the weight loss results in SELECT are bad compared to STEP 5. If this was some big conspiracy, Novo Nordisk wouldn’t be publishing the data with the lower % weight loss, right?
It’s also worth noting here that the lifestyle intervention in STEP 5 was specific to weight loss, while the lifestyle intervention in SELECT was not, so it makes sense that the weight loss in STEP 5 was greater than in SELECT (though, again, we’re talking 5% difference).
Claim: Statins are more effective at reducing cardiovascular risk than semaglutide.
Fact: I think it’s obvious that you can’t just look at a study of statins and compare that to semaglutide. I don’t know which meta-analysis the host refers to here that shows an absolute risk reduction of 4%, but from the way she described it, I don’t think she’s interpreting it correctly (also because of the previous error calculating the absolute risk difference in SELECT). For one, I don’t know what she means by a “five year meta-analysis” because meta analyses combine studies of different lengths. In my searches, I was unable to identify a meta analysis of the effectiveness of statins among adults with pre-existing CVD, though I did find several among adults without pre-existing CVD. This is, importantly, because statins are often used for primary prevention of CVD. So all of that is to say, we don’t really know this, but I do expect some indirect treatment comparisons will be coming soon because this is definitely a hot topic!
Claim: The FDA approved semaglutide for adults with “overweight and obesity”, but “that wasn’t really who that this trial was for.”
Fact: The FDA did not approve semaglutide for all adults with overweight and obesity. The FDA approval is for adults with overweight and obesity with cardiovascular disease.
Claim: After 2 years, only 25% of people are still taking semaglutide.
Fact: This number varies by source, but it is certainly true that long term adherence to semaglutide for weight loss is low. However, we cannot necessarily generalize that to the population with CVD. We’ll have to wait to see the research!
Claim: “A significant number of people got up to 2.4 but then titrated right back down again.”
Fact: Very few patients reduced dose after reaching 2.4 mg. You can see this in the graph below from the Appendix (p. 33). Confusingly, this is also in direct opposition to the host saying that people probably don’t even need to take this high of a dose (note that she is not basing that on any evidence or medical expertise). If she thinks that high of a dose isn’t necessary, why would it be a problem for the dose to be reduced for some people?

Claim: Intentional weight loss leads to earlier mortality in adults over 65.
Fact: There is no “strong body of research” showing that intentional weight loss over 65 is associated with earlier mortality. There are certainly some observational studies that suggest that, mostly from the 1990s or earlier, but there is also evidence from a randomized controlled trial that suggests otherwise. This is an incredibly complex research question and I don’t feel comfortable saying we have established this as fact either way. Especially because we do know that weight loss in that group is associated with improvement in metabolic health (ref 1, ref 2).
Claim: “I haven’t seen any research they’ve provided to suggest any better outcomes for people on this drug.”
Fact: I’m not sure what outcomes the host is referring to here, but the SELECT trial is quite literally research that shows that people on semaglutide have better CVD outcomes. There is also strong evidence that semaglutide reduces the risk of kidney failure and other clinically important kidney outcomes in patients with type 2 diabetes and chronic kidney disease. It’s possible the host just doesn’t believe any of the research and that is why she is saying this, but the research does exist!
Claim: Australia has “resisted” Novo Nordisk’s “attacks” because the Pharmaceutical Benefits Advisory Council told them it would be too expensive and “you haven’t provided us any information on whether or not this will improve health beyond just the weight loss stuff.”
Fact: This is a good place to clarify the difference between clinical approval, like through the EMA or FDA, and insurance coverage. This statement from the host is incorrect, because the Therapeutic Goods Administration (TGA), Australia’s FDA, has not yet approved semaglutide for cardiovascular disease (it is still under evaluation). So the Pharmaceutical Benefits Scheme (PBS) can’t even evaluate including it in the formulary. Wegovy isn’t included in the PBS for weight loss alone, but also Wegovy wasn’t even available in Australia until this month (August 2024). The host also says that Novo Nordisk has “paid the payback, $270,000 to get a private, facilitated workshop.” I’m not sure why the host is calling this a “payback”, but as someone who has actively participated in economic and clinical submissions to the Australian PBAC, I will explain the process in a bit more detail. Basically, if your initial submission to PBAC is rejected/denied, there are a few different resubmission options. One of those options is what is called “Facilitated Resolution Pathway”. There is indeed a fee associated with this, but it’s not a bribe or a payout or anything - it’s just the normal process. Of note, this pathway is only available if the treatment has been deemed “high added therapeutic value” (HATV). In the public documents from the November 2023 PBAC meeting regarding Wegovy, PBAC wrote, “The PBAC advised a facilitated resolution pathway would be appropriate given the high added therapeutic value of semaglutide and outstanding issues for resolution in defining the patients in whom treatment would reduce downstream consequences of obesity, be cost-effective, and appropriate for the significant Government expenditure.” In other words, contrary to what the host is implying here, PBAC believes that Wegovy is a high value treatment.
Claim: Russia has approved “bootleg versions of Ozempic to be sold.”
Fact: Russia is working on building out its own pharmaceutical industry. There is no “bootleg Ozempic” - it is a legitimate pharmaceutical company creating an analog of Wegovy (another source).
Claim: Novo Nordisk attempted to cover up the analysis about CVD risk and weight loss because the results were not what they wanted.
Fact: The results of this analysis are actually great for Novo Nordisk! I am not sure why the host is projecting a negative interpretation onto this. Think about it - this means that Novo Nordisk gets to recommend people stay on semaglutide even if they aren’t losing weight on it. Jackpot! If you want to be cynical about Novo Nordisk, the host’s interpretation makes no sense. This result is far better. Anyway, Novo Nordisk isn’t hiding anything.
In fact, the lead author, Dr. Deanfield, said, “Our findings show that the magnitude of this treatment effect with semaglutide is independent of the amount of weight lost, suggesting that the drug has other actions which lower cardiovascular risk beyond reducing unhealthy body fat. These alternative mechanisms may include positive impacts on blood sugar, blood pressure, or inflammation, as well as direct effects on the heart muscle and blood vessels, or a combination of one or more of these.”
It’s pretty awesome that this drug decreases CVD risk regardless of weight lost!
Concluding thoughts
There is so much misinformation circulating on the internet these days, and it can be really difficult to figure out who to trust. For podcasts like this, I encourage people to look at the qualifications of the individuals who are purporting to be experts, and to question if they really have the relevant experience and knowledge to be speaking with such authority. In this case, the answer is a resounding “no”. Maybe you read this whole post, maybe you didn’t - I know parts of it were quite dry and parts were a bit technical, but I hope at least it helped clarify some pieces of the misinformation about semaglutide that is rampant in certain circles of the internet.
I also want to take this opportunity to recommend a recent episode of Sigma Nutrition about correlation/causation. It’s very well done, and effectively communicates the same thing that I wrote about, only more articulately and in more detail. 🙂
Thanks for reading!
The Return of the King
Thank you for this!
So much of the coverage of semaglutide is either entirely too fawning and surface-level or too conspiratorial in tone, so I really appreciate you doing this!