


Maintenance Phase Reality Check: Zombie Statistics Spectacular!

About me/why you might trust my analysis: I have a PhD in epidemiology and health economics, and I currently work as a biostatistician. As a result, I have a deep understanding of study design and statistics, as well as the worlds of academia and research.
Before I start, I want to reiterate three things that are important for me to state before all of these fact-checks:
Fat-phobia is rampant, especially in the medical world, and causes significant mental and physical harm. Being fat is not a moral failing. Fat people should not be treated differently than “straight-sized” people.
Weight alone is not an indicator of overall health. Full stop.
There is still so much we don’t know about how adiposity and body composition impact human health. In order to make progress in this space, we need to abandon the entrenched anti-fat bias.
I have had some die-hard MP fans try to imply that my intentions in fact-checking MP episodes are not “in good faith” and question why I am “targeting” MP instead of the myriad other sources of misinformation on the internet. My answer: this is personal to me! I have friends and family who repeat the things they hear on this podcast thinking that it is accurate. They trust Aubrey and Michael, or did, until I showed them just how bad so much of this content is.
In this particular episode, Michael and Aubreyl go beyond just misinterpreting science and actually enter a dangerous anti-science realm, including saying that women get gallbladder cancer from dieting (not true at all) and that we don’t know anything about what causes diabetes (we do). This episode is also a really good example of the poor research that Michael and Aubrey do, despite some die-hard MP fans telling me that the research they do is “impeccable.” Michael even admits to not knowing some pretty basic facts about the studies he is reporting on. There are also numerous examples in this episode of them completely misrepresenting what the academic world believes.
I find myself wondering what Aubrey and Michael want to achieve with this podcast. Putting out this kind of anti-science misinformation is really harmful to the human rights social movement for fat acceptance because it gives the other side more fodder. The misinformation in MP episodes is being weaponized by people who promote disgusting fat phobic views. A very articulate redditor said, “In all seriousness though, misrepresenting the science to make your argument about anti-fat bias does a disservice to the entire movement. If the left/progressive folks don’t hold each other accountable and uphold a culture of journalistic integrity in their activism, then we’re really no better than people on the right who make bad faith arguments to push their agenda.” So yeah, that's why this is important to me.
Thoughts on science communication:
I think it’s safe to say that the state of scientific communication is poor. Between scientists failing to articulate research findings in an appropriate way and media companies reaching for sensationalist headlines, health and science news is really a mess. What Aubrey and Michael are doing with MP is portraying “science” and “public health” as monolithic entities that lack nuance and self-reflection. This is patently false. There was a really great article in 2007 by two sociologists at UCLA, Saguy and Almeling, called “Fat in the Fire? Science, the News Media, and the “Obesity Epidemic” (if you can’t access it, let me know and I can send you the PDF). Here is a very powerful quote from the conclusion:
Our analyses suggest that the news media take their cue from scientific studies when it comes to representing obesity as a crisis, but that they also throw ‘‘fat on the fire’’ by using—more than the scientific studies on which they report—evocative words like ‘‘epidemic’’ or ‘‘war.’’ By referring to extreme examples as illustrative of the larger category of ‘‘overweight’’ or ‘‘obese,’’ the news media magnify the perceived extent and scope of the ‘‘obesity epidemic.’’ The news media are more likely than science to ascribe individual blame for weight.
Aside from the rampant misinformation and incorrect interpretations of scientific studies, Michael and Aubrey are barking up the wrong tree.
Why are they not tackling media claims by returning to the science and seeing what the science actually says?
Why do they try to “debunk” science when they don’t have scientific backgrounds?
Why don’t they invite experts on, when they don’t have the requisite experience to address things they want to explore further in the science?
The article I linked to above also calls out the media and journalists for not questioning the scientific studies. I think that is what Aubrey and Michael are trying to do, but they aren’t actually questioning anything, they are just claiming that things are wrong without having the background to appropriately assess the research. Saguy et al. wrote, “We find that journalists are more likely to report on articles that lend themselves to dramatization than on those that do not.” Michael and Aubrey fall prey to this, as well, and further the problem by implying that ALL articles are like those they choose to report on. I don’t need to explain why this is dangerous.
I’ll leave you with one final quote from Saguy et al.: “Do journalists, in turn, function as ‘parascientists’? No, if the definition of a parascientist involves independently evaluating research studies.” Michael and Aubrey, as media personalities, need to recognize their limits and allow experts to comment on the science. There are tons of experts, many who are part of the fat-acceptance movement, who they could lean on. If they really want to make change, they should be harnessing all of the resources available, not spreading misinformation that fat-phobic trolls can weaponize against the movement.
Ok, on to the episode:
The reason for all of this is that, while I was reading Michael Pollan's book, in the first chapter, he has a five-paragraph section, where he talks about like the ravages of obesity.
Just a quick note that the section that Aubrey reads right after this is from Chapter 6, not the first chapter, in case anyone is curious. It’s also missing a piece. The full first sentence is, “The alcoholic republic has long since given way to the Republic of Fat; we’re eating today much the same way we drank then, and for some of the same reasons.” Not that important, but just wanted to point this out.
I am most curious about this cost to the healthcare system number. I feel there are different numbers that get thrown around and they are always in the billions… I have no earthly clue, where those numbers come from. I have no earthly clue, why they're different every time.
This would be a fantastic opportunity for Aubrey and Michael to have a guest host who is a health economist. In lieu of that, I will do my best to explain where these numbers come from and why they vary from one study to another. First, consider that all of these numbers are estimates. There is no giant database that contains all the healthcare expenditures in the United States and whether or not they are due to obesity. So researchers are piecing together data sources, and different researchers use different sources! A common way that the numbers specifically for obesity are estimated is by calculating the “population attributable risk” (PAR) which is the portion of cases of a disease in a given population that is considered “due to” the exposure to a risk factor (in this case, obesity). The equation is:
PAR = (Incidence in total population) – (Incidence in unexposed group)
The PAR is converted to a proportion and applied to the prevalence of a condition of interest to calculate the number of cases due to the risk factor. Then that number of cases is multiplied by estimates of the cost of treating/managing the condition. So you can see here that the ultimate cost that comes out of something like this is dependent on the estimated incidence (which can vary across studies) and the estimated cost of treating the condition (which also varies across studies). The aggregate cost for something like obesity would also differ depending upon which conditions are included in the estimate (e.g., diabetes and asthma or just diabetes?). Unfortunately, this isn’t an exact science - it’s a process of estimating using what the researchers perceive to be the best available data. Hopefully that sheds some light on why these estimates vary!
-they appear on the surface as if they fulfill an informational function. It's like, "Oh, a piece of information, right?" I learned how much America spends on obesity every year. But what they're actually doing is serving a rhetorical function. Because that number is utterly meaningless. $90 billion a year. Okay, how much do we spend on healthcare total? How much do we spend on cancer every year? That number could be $45 billion and that number could be $500 billion, and you'd probably have exactly the same reaction. You'd be like, "Wow, that's a lot."
This is a common tactic that MP uses to make things that are totally reasonable seem outlandish or absurd. Of course, what Michael is saying could be said about any number that doesn’t have context, and is why it is placed alongside the percent of healthcare spending this accounts for. These numbers are not utterly meaningless and they don’t serve a rhetorical function.
This just sounds like an astronomical amount. There're so many judgment calls that go into this. The assumption here and the way that it's deployed is, fat people are costing you $90 billion. Think about what you personally could do with $90 billion… It’s not explicit, but the implicit message is really clear, which is it's fat people's fault.
I think it’s really important to take a step back when statements like this are made. Is fat-phobia rampant in our society? Absolutely. Is every piece of data about fat people being used as a weapon? No. It is really harmful to the fat acceptance movement to turn things like this into a problem when they are not. Health economists estimate the cost of care for many many many types of things: cancer, diabetes, injuries, even being “underweight”! This is what health economists do. It is not blaming fat people. Michael and Aubrey are taking this out of context as if this type of thing is ONLY done for obesity.
The primary way that you can tell that nobody cares about these numbers or where they come from is that, Michael Pollan uses the wrong number.
See below. Michael Pollan does not use the wrong number. However, Michael DOES use the wrong numbers below. Make of that what you will.
This appears to come from a 2004 paper called The Escalating Pandemics of Obesity and Sedentary Lifestyle… This actual study finds that the costs are $70 billion, but then it cites a 1995 study that found $99 billion dollars. Somehow $99 billion became $70 billion became $90 billion in Michael Pollan's book.
This is all false. The abstract of this paper says: “These intricately linked conditions are responsible for an enormous burden of chronic disease, impaired physical function and quality of life, at least 300 000 premature deaths, and at least $90 billion in direct health care costs annually in the United States alone.” We can assume that is where Pollan got the $90 billion figure. That $90 billion comes from the 1999 (not 1995) paper that “estimated the direct cost of obesity in the United States at $70 billion (in 1995 dollars using a definition of obesity as BMI ≥30) and the direct cost of inactivity at $24.3 billion (using 28.8% as the proportion of adults reporting no leisure-time physical activity).” This is very explicitly stated in the body of the 2004 paper. The 1999 study does not report the number $99 billion anywhere. It is clear that $90 billion comes from $24.3 billion + $70 billion.
It says, "In the absence of obesity, Medicare and Medicaid spending would be 9% and 12% lower respectively." … Which also, A, sounds like a bargain. Secondly, you can find records from the 1960s that show that 12% of the US was "obese" according to current BMI statistics. In the 1960s, 35% of the country was "overweight" as well. So, in the absence of obesity, when the fuck are we talking about it? Like the 1300s?
Michael is either being intentionally obtuse or he really doesn’t understand the fundamentals of this kind of research. No one is literally talking about a time when obesity didn’t exist. It is the same as saying, “in the absence of cancer…” It’s just language that conveys that these costs are attributable to a certain thing. This is called a “counterfactual” and it is a central concept in epidemiology.
But then, okay. This is just conceptually gross and shouldn't exist. But of course, as part of my rabbit hole tumbling, I started looking at the other numbers, because as we noticed with this number itself in Michael Pollan's book, there's no consistency. These numbers bounce all over the place. I started looking at the canonical "costs of obesity," throughout time. The earliest I could find was 1990, a study estimated the cost of obesity at $46 billion… There's a 1994 paper that says $70 billion. There's a 1998 paper that says $78 billion. There's this 1999 paper, the Pollan references that says $99 billion. So, from 1990 to 1999, the costs of obesity have somehow doubled. They've gone from $45 billion to $99 billion.
Again, the 1999 paper that Pollan references says $90 billion, not $99 billion. I don’t know where Michael is getting that number. This is where it might be helpful if the podcast cited its sources, but Michael is conflating things and not reporting the results of these studies correctly. The 1994 paper, “The Cost of Obesity” reports the cost of obesity in 1990 dollars as $68.8 billion. There is no 1990 paper that reports $46 billion. That same 1994 paper reports the direct costs of obesity in 1990 as $45.8 billion. Again, this is a single paper and the results of that study say the total (indirect and direct) cost is $68.8 billion. There is no paper that says that the cost of obesity is $46 billion. So actually, we’ve gone from $70 billion to $90 billion which is pretty much a margin of error in studies considering inflation ($70 billion in 1990 is equivalent to $81.6 billion in 1995) and that these are estimates. This is not a whole confusing mess. It’s all actually quite consistent!
Aubrey: Can I take a swing at one of the factors?
Michael: Oh, do it.
Aubrey: The definition of obesity changed.
Michael: Oh, yeah. I know.
Aubrey: You lowered the floor for who you consider fat and then you're like, "Fat people cost us so much money" and didn't mention we have millions more people who are now medically defined as fat, because we changed the definition.
Nope. Both the 1994 and 1999 papers used a cut off of 29 kg/m^2.
We're now at $99 billion in 1999. There's then a 2008 paper that says $147 billion, a 2016 paper that says $261 billion and another 2016 paper that says $481 billion.
Again, we’re at $90 billion in 1995, not $99 billion in 1999. I have no idea what papers Michael is talking about here, but here is a 2016 paper that reported that in 2008, “the aggregate national cost of overweight and obesity combined was $113.9 billion.” This is, again, not surprisingly different from $90 billion in 1995 dollars given inflation and given that this paper is aggregating obesity and overweight whereas the 1999 paper was only looking at obesity. A meta-analysis from 2016 reported that obesity was estimated to account for $149.4 billion in 2014 dollars. Again, not that different from what we’d expect due to inflation, a growing population, and rising rates of obesity. I highly recommend reading that meta-analysis, as it delves into how the different methods impact the resulting estimated economic burden. If you dig into the literature here, you’ll find a wide variety of estimates. Michael has just chosen a handful that support the message he wants to convey that these estimates are rising at an absurd rate. Remember that not all studies are created equal, and finding a study that has an outlandish result doesn’t mean that the scientific community trusts it or pays attention to it nor that it is reflective of the larger body of literature on the topic. As an aside, the $481 billion comes from a 2018 Milken report (not 2016) which is not a peer-reviewed paper.
I found a 2016 meta-analysis that looked at 23 different estimates of the costs of obesity over time. It's actually a fascinating article, because it has this deep air of confusion, where they look at all of the different methodologies that people use and everyone basically does the same thing. They basically look at various health conditions and they'll say, "Okay, obesity accounts for 40% of this one, and 60% of this one, and 90% of this one," and then they count up the costs. There's this Medicare survey thing of like, "How much America spends on pancreas cancer every year? How much America spends on elbow pain?" It's this whole list of costs and then you just do the math. They're all using essentially the same structure to come up with these estimates. But what this meta-analysis finds from 23 studies, some of them include 30 cancers and some of them include one cancer. This is from the review. It says, "Musculoskeletal disorders were considered in nine studies, respiratory disorders in six, and digestive diseases in five studies. Four studies included mental disorders such as depression."
This paper is from 2017 and is not a meta-analysis. It is a systematic literature review of papers that were published from 2011 to 2016. There was no meta-analysis performed. It is really confusing to me how consistently Michael gets the dates of papers wrong. Anyway, I am not sure why Michael chose this paper, as it was published in a pretty random journal, it has a very limited scope, and it’s not particularly well done. There are tons of really well done studies on the economic burden of obesity, but Michael chose this single study. It is really important to highlight that one of the stated objectives is to “identify and describe different obesity-related diseases included in the selected studies.” The introduction explicitly states “In addition, none of the reviews has systematically analysed the obesity-related co-morbidities included in the cost calculation. Since obesity itself is not only a disease but also a risk factor for other diseases, it is important to study which co-morbidities have been included in the different COO analyses. The attributable burden of obesity differs across studies. Attributable burden is determined by the co-morbidities included in a cost calculation. It would be interesting to examine how, in the included studies, these co-morbidites are adjusted for in the overall cost calculation.” Michael presents this as if it is appalling, and as if it just appears out of nowhere in the results, but it’s VERY clear from the outset that the study is going to do this. Michael’s reaction to it is perplexing. This is akin to going to a bookstore, selecting a romance novel, and then acting shocked when it contains sexual content. There are tons of published papers on the economic burden of obesity that do not include “obesity-related diseases.” This is a common occurrence in MP episodes - they find a single study that they find objectionable and present it as if it is a huge problem in science. As an aside, I have no idea what he means by “it has this deep air of confusion.” It doesn’t seem confused to me at all. They are very clear about what they are going to do and then they do it. Perhaps it is just Michael who is confused.
There's no way to make the claim that it's caused by obesity. Again, it's just this cluster of correlations. We've talked about this a million times. People with less education are more likely to get various cancers and heart disease. People who have never been married are more likely to have high mortality rates. People who live in Massachusetts live 10 years longer than people, who live in Mississippi, where all of us are these bundles of correlations based on various demographic characteristics and what they're doing is, they're putting obesity basically at the top of that list. Obesity is the most important thing.
Actually, there are ways to make that claim. There are biological mechanisms that can explain a lot of the causal relationships between obesity and certain diseases (not all of them, though). In contrast, there isn’t a biological mechanism that explains how lower education status increases risk of cancer or heart disease. No one is saying obesity is the most important thing, but this is a paper about obesity, so of course it is focusing on obesity. Again, this is like reading a report about opioid misuse and then saying everyone only cares about opioid misuse, not all the contributing factors. You have chosen content that is about obesity. That is why it focuses on obesity.
There's a think tank report in 2016. This is the one with the highest estimate of the cost of obesity. This is $481 billion a year. I actually appreciate them doing this. They list 23 conditions and the various risk rates for fat people and for nonfat people. One of the ones they list is Alzheimer's, that apparently fat people are slightly more likely to get Alzheimer's. They then say that fat people are responsible for 29% of the healthcare spending on Alzheimer's every year.
Again, this is a 2018 report. Also, the report does not say that 29% of healthcare spending for Alzheimer’s is due to obesity. In fact, there is no mention of 29% in this report. This number is entirely made up by. EDIT: I originally wrote, “In the 2020 report, Milken estimates that 6% of the costs of Alzheimer’s are due to obesity (see graph from the report below)”, but a very astute commenter pointed out that actually the pie chart below suggests that 6% of the total costs associated with obesity are due to Alzheimer’s, not the other way around. Thanks to the commenter for the correction! As an aside, Michael is being intentionally crude with his language here as a way to rage bait. The reports don’t say anything about fat people being responsible for spending. These costs are based on calculations of population attributable fractions (the methods are very clearly spelled out). Milken is not assuming that all of the conditions are due to obesity. Michael is either playing dumb to get people worked up, or he didn’t read this report at all.
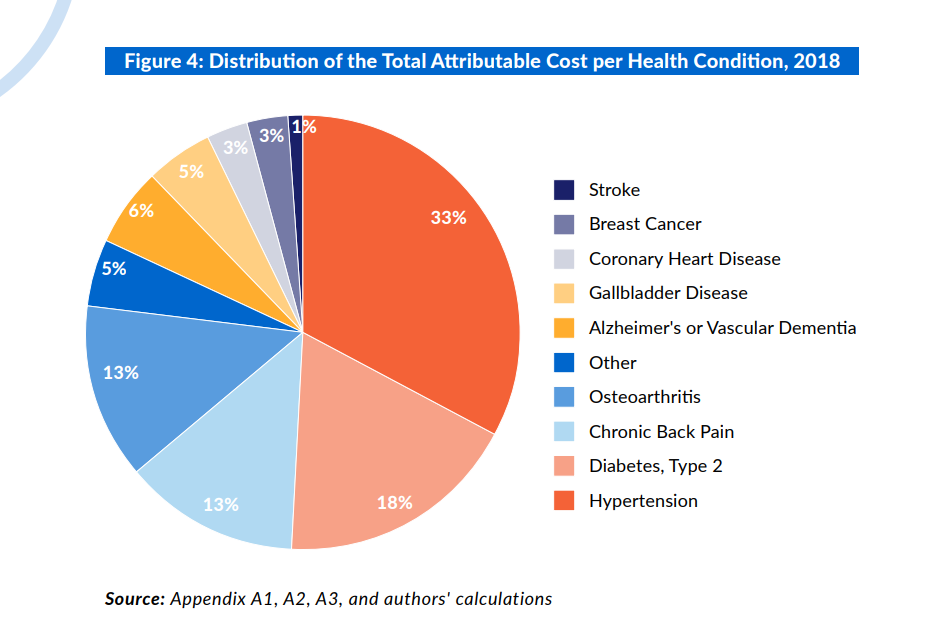
It's not 100%, but they are attributing a huge percentage of healthcare conditions to obesity without actually looking into any of the actual complexities of these. The one that I really got stuck on, one of the ones in this analysis is gallbladder cancer, that fat people are more likely to get gallbladder cancer than thin people, fine. There're 8,000 cases of gallbladder cancer every year and they're attributing 4,000 of them to obesity. 4,000 cases of gallbladder cancer are like obesity-related gallbladder cancer. But then you start looking into gallbladder cancer, first of all, as we've discussed before, one of the risks of gallbladder disease, which is a precursor to gallbladder cancer is dieting. Because when you rapidly switch to a low calorie or low-fat diet, your internal systems go haywire and you're producing all this bile, and that puts more stress on your gallbladder system.
A lot of misinformation here. First, “dieting” is not a risk of gallbladder disease. While rapid weight loss (>1.5kg per week) and gastric bypass surgery increase the likelihood of developing gallstones, losing weight at a healthy rate decreases the risk. It is dangerous and irresponsible of Michael to suggest that “dieting” (an incredibly vague term) increases the risk of gallstones, let alone gallbladder cancer. Also, I know that this isn’t a science podcast, but there are ways to communicate medical phenomena in layman’s terms that are correct and promote health literacy. Saying “your internal systems go haywire” which puts “stress on your gallbladder system” is wrong, and not just because it is a simplification of a complex process. It’s just wrong. Here’s a very simple explanation: Gallstones occur primarily due to 1) having too much cholesterol in your bile, and 2) bile sitting in your gallbladder for too long (“stasis”). When you are eating a very low calorie diet without enough fat, your gallbladder doesn’t have a reason to release bile, so the bile just sits in your gallbladder and turns into sludge. This, along with increased cholesterol in the bias due to rapid weight loss (>1.5kg per week), increases the likelihood of gallstones forming. These are actually exactly the same mechanisms underlying the relationship between obesity and gallstones! Obesity is associated with decreased bile duct motility and increased cholesterol in the bile. Decreasing body weight in a healthy manner reduces cholesterol saturation and therefore reduces the risk of gallstones.
To put to rest Michael’s inappropriate implication that dieting causes gallbladder cancer, I’d also like to point out that it is really unlikely that gallstones that occur in people who have lost weight quickly would put them at increased risk of gallbladder cancer. Why? Because it is chronic inflammation that is the problem. While research suggests that gallstones can develop with rapid weight loss (not commonly, however), that is not the same as having chronic gallstones - we know (see sources above) that the risk of gallstones decreases with (healthy) weight loss. Additionally, the risk of gallbladder cancer is very low. A huge population-based study from Sweden looked at all the patients who received cholecystectomy (removal of the gallbladder) and reported that only 0.6% of them had gallbladder cancer.
Women are three times more likely than men to get gallbladder cancer, which I'm not going to say dieting is 100% of the reason for that, but women are also more likely to diet than men.
We know why women are more likely to get it. It’s hormones, not dieting. See above for explanation of why dieting would not be the cause here. It’s very irresponsible for Michael to imply that dieting has any impact here. There are no studies linking “dieting” to gallbladder cancer.
A small selection of sources (note that all of the studies of gallbladder cancer are based on small numbers because it is a rare cancer):
Well, also, one thing that you find throughout these lists in this study and in other studies is that what they call the cost of obesity is actually the cost of discrimination against fat people. One of the interesting things about gallbladder cancer is, it almost exclusively happens in people between 85 and 89 years old… Yeah. It's a very rare cancer and it's almost always fatal, because people don't really get tested for it and it's oftentimes diagnosed really late. First of all, we know that at higher ages above 70, fat people actually have lower mortality rates than thin people. We're not entirely sure why, but it's actually protective to be fat in old age. We also know that fat people are less likely to seek medical care and they're less likely to get scans that they need. Oftentimes, they go in with some sort of symptom and their doctor says, "Eh, come back when you've lost 50 pounds." Some, I'm not going to say all, but some of the higher cancer rates for fat people are actually because they're not getting high-quality medical care and they're not getting tumors taken out of them when they need to.
Several things to address here. First, mortality rates for fat vs thin older people have nothing to do with this. I’m not sure why Michael brought this up. We also know that being fat is not “protective” - this is not a causal relationship. They have discussed this multiple times before, so I’m not sure why he is reversing course here, except that it fits his narrative.
Second: it is incorrect that gallbladder cancer “almost exclusively happens in people between 85 and 89 years old.” The median age at diagnosis in the US, according to SEER, is 71. I understand that a lot of people think that it’s not a big deal that MP gets these facts wrong, but it seems like a pretty big red flag when the hosts can’t get basic facts right that they could easily Google.
Third: another place where an expert host could have helped here is that there isn’t a test for gallbladder cancer. It’s not like breast cancer or cervical cancer where there is routine screening. It’s almost always diagnosed incidentally and is asymptomatic. That’s why it gets diagnosed late - because there is no reason it would have been found earlier. In fact, it is often diagnosed as an incidental finding during gallbladder removal (cholecystectomy). So while there is a lot of discrimination against fat people in the medical world, this particular case is not an example of fat people “not getting tumors taken out of them when they need to.” It is important that we acknowledge when there is solid science underlying the association between adiposity and disease. That’s not counter to the mission of fat acceptance. If we ignore these things, or say they aren’t true, we are doing a disservice to fat people. Imagine, instead of Michael and Aubrey claiming that being fat isn’t actually a risk for gallbladder cancer, if they said, “hey, we should screen high risk fat individuals for gallbladder cancer to improve health outcomes.”
Right. Well also, one thing that I got really frustrated by looking into gallbladder disease specifically was how few studies look at anything other than obesity. I found a relatively small study in Iran that looked at 300 women with gallbladder disease and actually asked them a much wider range of questions about their lives. This is from the study. It says, "Having three or more births, increased the risk of gallstones by more than five times followed by having rapid weight loss, being single, having familial history of gallstones, and consuming high total energy." So, okay, there's some eating behavior stuff in there, but it's the fifth best predictor. And then the best predictor turns out to be having three or more kids… Part of the problem here is, first of all, it's just really easy to do obesity studies, because the data is available. Then you can ask people like, "How tall are you, how much do you weigh?" Okay, boom data point. And then you can link that to whatever health outcomes they have. But it's much harder to get a broad picture of the predictors of a disease in a more qualitative way. This is a small study. It's only in Iran. I'm not going to say that like, "Oh, it's actually births that are predicting this better than anything else," because I think that would be just as shallow as saying it's like a cost of obesity. But also, I don't think the data supports the conclusion that if there were no fat people. We would save half of our healthcare spending on gallbladder cancer every year. I didn't look into the other 22 conditions and costs on this list. But to me, this whole exercise feels as superficial as saying, "Well, if everybody who lives in Mississippi moved to Massachusetts, they would all live 10 years longer."
First, Michael is entirely misrepresenting this study. I think he just read the abstract. This study is not even about what he says it is. The sentence he is citing is from the abstract and is referring to unadjusted analyses. In other words, correlation, not causation. It’s just a crude comparison of cases (women with gallbladder disease) vs controls (women without gallbladder disease). Also, women were excluded from the control group if they had a history of dieting, while that same criterion was not applied to cases. So the difference in “history of rapid weight loss” is an artifact of the sampling schema. Anyway, the actual objective of this paper was to assess “the association of dietary patterns with gallstone disease.” When adjusted for confounding factors (education, occupation, marital status, number of live births, physical activity, energy intake, calcium supplementation, family history of gallstones, and history of rapid weight loss), women who had gallbladder disease (cases) had an 86% lower odds of being in the top half (above the median) of consumption of what the researchers deemed a “healthy dietary pattern” and had an almost 4 times higher odds of being the top half (above the median) of consumption of what the researchers deemed an “unhealthy dietary pattern.” You can see that this is a pretty uninterpretable study. It was exceedingly poorly done.
Second, I am not sure why Michael chose this study. In addition to being a very poorly done study, it was published in a really obscure journal. It’s also not about gallbladder cancer, it is about gallbladder disease. As I stressed before, the risk factors for gallbladder disease are not the same as for gallbladder cancer. So this paper is irrelevant. It is also full of all of the methods that Michael and Aubrey call out as problematic in other contexts. It is self-report and used food frequency questionnaires. If this study said that obesity was the primary risk factor for gallbladder disease, he would be ripping it apart. MP often picks a single study that fits their narrative and presents it as if it is representative of all literature on a topic. What’s most ironic is that this study didn’t even look at obesity! Michael is using a study that didn’t look at obesity as a risk factor for gallbladder disease to try and argue that all of the studies look at obesity because it is so easy to measure.
Third, Michael is using another straw man argument. There are tons of studies (see those I linked above) looking at other risk factors for gallbladder cancer (and pretty much every disease). Michael is specifically looking at obesity research. That is why he is finding studies looking at obesity (except, apparently, this one).
Michael: This is where we get into the shit about lost productivity.
Aubrey: What?
Michael: Some of these studies include lower wages.
Aubrey: What?
Aubrey: We pay you less and now that's a cost we shoulder?
Michael: That's fucking ghoulish, dude. To be like you earn less money, therefore I'm paying extra for you.
Either Aubrey and Michael are being intentionally obtuse, or they really don’t understand what they are talking about here. It is important to realize that these papers about economic burden are estimating costs to the US economy. Not costs to a single person. Therefore, lost wages ARE relevant. It’s not about paying folks less, it’s about lost wages due to illness or other responsibilities (childcare, elder care, etc.). This is common in the health economics literature and is very very important to incorporate to get a full picture.
Michael: One of these studies I found also, because there's like absenteeism that people lose X number of days a year of work due to their health condition, like, that's part of the cost. But the problem with fat people is that, there's no evidence that fat people miss more work than thin people. One of the studies I found, the disappointment is palpable. They're like, "Oh, yeah, we can't actually count up last days of work due to obesity." So, they count fucking presenteeism.
Aubrey: Wait, what? They count when you're there as a cost?
Michael: You are just hanging out at work, I guess. [laughs] I don't know what fucking survey this was. But I guess fat people are some percentage more likely to admit to being presentiest at work. That's considered a cost of obesity. Try to devise something that I am less interested in.
Whether or not fat people miss more work than thin people is irrelevant here. For those who don’t know, presenteeism is basically showing up for work but not being at “full capacity”. In other words, it’s being at work without 100% productivity. This is a standard thing to look at in health economic literature. Instead of saying “I don’t know what fucking survey this was”, Michael could have looked into the literature, at the many examples of how presenteeism is assessed, and specifically the presenteeism reported among fat folks. Here is a study that reports on several examples that you can look through (see the presenteeism section): Productivity loss due to overweight and obesity: a systematic review of indirect costs - PMC (nih.gov). For people who don’t want to read it, presenteeism is measured via questionnaires, usually the Work Limitations Questionnaire. In other words, these studies are using data collected from the workers themselves who report that they have difficulty performing the work.
Also, think about, I could sit down and I could make a cost of thinness. How many tens of millions of dollars do we spend on weight loss? How much loss productivity is there when somebody is in the throes of an eating disorder? Think you could easily do some try hard index about the cost of thinness to America. But that doesn't really mean anything. None of us actually think in this way. Some of these studies include fucking transportation costs that jets have to use more fuel, because they have more fat passengers now.
This is a rhetorical fallacy that we call a “red herring.” It is entirely irrelevant to the topic at hand. There are studies that look at this. Here’s one: Social and economic cost of eating disorders in the United States: Evidence to inform policy action - Streatfeild - 2021 - International Journal of Eating Disorders - Wiley Online Library. Here’s another: Household expenditures on dietary supplements sold for weight loss, muscle building, and sexual function: Disproportionate burden by gender and income - PMC (nih.gov). Again, Michael is specifically looking at literature for obesity. That is why he is finding obesity studies. Also, yes, health economists and policymakers DO think this way. That’s what the field of health economics does!
It's also even in the direct healthcare spending, when you look into it, there's actually, basically no difference between fat people and thin people, and things like the time they spent as doctors, the number of surgeries they have. Almost all of the actual difference in costs between fat people and thin people is prescription drugs. Fat people are more likely to be taking statins, they're more likely to be taking metformin for diabetes. The obvious solution to that would be to make the prescription drugs cheaper.
There is a large body of literature that contradicts these statements - including ones that Michael mentioned earlier in this episode. Since Michael did not cite any sources here, it’s very difficult to know where he is finding this information. Anyway, here are some recent ones that do not support his assertion:
Direct medical costs of obesity in the United States and the most populous states - PMC (nih.gov) - “The effects of obesity raised costs in every category of care: inpatient, outpatient, and prescription drugs.”
Healthcare costs attributable to abnormal weight in China: evidence based on a longitudinal study | BMC Public Health | Full Text (biomedcentral.com) - “In 2018, healthcare costs per person for overweight and obese population were estimated to be $607.51 and $639.28, respectively, and the underweight population was $755.55.” Note that this is in China, a country with much much lower drug prices (somewhat irrelevant since Michael’s comment about prescription drugs is wrong, anyway).
Association of body mass index with health care expenditures in the United States by age and sex - PMC (nih.gov) - “Among adults, obesity was associated with $1,861 (95% CI $1,656-$2,053) excess annual medical costs per person, accounting for $172.74 billion (95% CI $153.70-$190.61) of annual expenditures. Severe obesity was associated with excess costs of $3,097 (95% CI $2,777-$3,413) per adult.”
Health care costs and lost productivity costs related to excess weight in Belgium - PMC (nih.gov) - Note that this is in Belgium, also a country with much lower drug prices (again, irrelevant given that Michael’s comment is wrong, but still worth noting as evidence that his point is wrong).
Michael: But that's not what anyone is actually talking about. These paragraphs of like, "Obesity cost the US healthcare system a billion a year." That never leads to therefore everybody should get medical coverage and we should make prescription drugs free. It leads to "Everybody should lose weight."
Aubrey: All roads lead back to, we actually need universal healthcare and that is a thorny, hairy, challenging problem that nobody fucking wants to take on and it is way the fuck easier to just be like, "Fat people cost so much money. Let's be mad at them about it" rather than being like, "Okay, let's get together another strategy on this issue that never dies."
This is a fundamental misunderstanding of economics. The cost to the healthcare system would not be lower if we had universal healthcare. Someone has to pay for these things - it’s not about the out-of-pocket costs for individuals, it’s about costs to the system. And even in countries with socialized medicine and lower drug prices, obesity is still associated with higher healthcare costs. See the examples I provided above.
A couple of things for people to know. One, eating sugar does not give you diabetes. We don't know what causes diabetes, type 1 or type 2. Thing two is, there is not really evidence that it's something that people "do to themselves" and there's a little bit of evidence that shows that actually weight gain might be the result of getting diabetes, not the other way around.
There are definitely still things that we don’t know, but we actually do have a pretty good grasp of what causes diabetes:
Type 2 diabetes develops when β-cells fail to secrete sufficient insulin to keep up with demand, usually in the context of increased insulin resistance. A minority of people diagnosed with type 2 diabetes also have evidence of islet autoimmunity (57,58). Obesity is a major risk factor for type 2 diabetes (59,60) with complex genetic and environmental etiology.
Insulin resistance develops with ectopic fat deposition in the liver and muscle. Fat may also accumulate in the pancreas and contribute to the decline in β-cell function, islet inflammation, and eventual β-cell death (61). Type 2 diabetes occurs at different levels of BMI/body fat composition in different individuals and at lower BMI for Asians and Asian Americans (62). For susceptible people, there may be a personal “fat threshold” at which ectopic fat accumulation occurs, worsening insulin resistance and resulting in β-cell decompensation.
Weight loss improves insulin sensitivity in liver and skeletal muscle (63) and may also reduce pancreatic fat accumulation (64). Defects in insulin secretion are at least partially reversible with energy restriction and weight loss in prediabetes and recent-onset type 2 diabetes (65). Unfortunately, it is difficult to reverse long-standing diabetes, even with the large weight loss associated with bariatric surgery (66).
Both reduced sleep time and increased sleep time are associated with the development of obesity and diabetes. Obstructive sleep apnea reduces sleep time and sleep quality and is associated with type 2 diabetes and metabolic syndrome. The modern “24-hour culture” may reduce sleep time and thereby also contribute to increased risk of type 2 diabetes. And while associations with additional environmental factors exist, there have been no direct causal relationships defined to date.
Research Gaps
There is a clear correlation of environmental influences to diabetes risk. Yet, the assembled experts agreed that hypothesis-driven research is needed to define direct causal relationships between specific environmental factors and pathophysiologies leading to diabetes. Research efforts need to address environmental etiologies of type 1 diabetes and determine their relative contribution to onset of autoimmunity and progression to symptomatic disease. Whether there is a direct causal role of the intestinal microbiota in pathogenesis of type 1 and type 2 diabetes and response to therapies needs to be determined. Public health interventions that successfully reduce the levels of consumption of energy-dense foods and/or reduce sedentary time and increase time spent in physical activity need to be evaluated to determine whether they can reduce type 2 diabetes incidence at a population level.”
Aubrey is correct that eating sugar does not give you diabetes, but it is well-established that diet quality has a significant impact on the risk of Type 2 Diabetes (so much so, that I don’t even know which articles to provide as references here. There are too many! Here is one good overview, though.) There is a large and rigorous body of evidence confirming the biological mechanisms connecting excess adiposity to diabetes risk. This is not up for debate.
References:
It's just this weird moment, where everybody's walking around, all of these people who do not have this incredibly complex, misunderstood chronic health condition are walking around like they own the place and they know everything about how not to get this chronic health condition. They know everything about how to treat it and prevent it. And honestly, most of the advice that people give and get around this is garbage, and it doesn't fucking work, and it bears no resemblance to any existing science.
This is dangerously anti-science. We know a LOT about diabetes, not everything, but a LOT (see all previous references). And we for sure do know how to treat it, and it is founded in rigorous science. I don’t know what Aubrey is trying to accomplish by suggesting that diabetes is misunderstood, but for anyone who needs to hear it, we do know how to treat diabetes! Please visit the American Diabetes Association website for more information.
The first identification of the difference between these two forms of diabetes was in 500 BC in India. The test for diabetes was they would have pee on the ground and if the ants crawled toward your pee, because pee is sugary, then you had diabetes and if they didn't, then you didn't have diabetes.
Incorrect. Diabetes was first identified in 1500 BC in Egypt (another source here). What Michael is referring to occurred in 500 AD, not BC. Here is a quote from the source I referenced before: “The association of polyuria with a sweet-tasting substance in the urine was first reported in Sanskrit literature dating from the 5-6th centuries AD at the time of two notable Indian physicians Susruta and Charuka. The urine of polyuric patients was described as tast- ing like honey, being sticky to the touch and strongly attracting ants. Indian descriptions of this time appear to distinguish two forms of diabetes, one affecting older, fatter people and the other thin people who did not survive long.” Note that the Wikipedia page gets this wrong, which is likely where Michael got this misinformation (don’t use Wikipedia as your source of information without checking the facts!!).
We've known the difference between type 1 and type 2 diabetes, since we've known about diabetes, basically. But essentially, we didn't really have a clear understanding. We didn't know what insulin was until very recently. We didn't understand the actual mechanisms. People call them a million different things. One of the terms was quick and thin diabetes versus fat and slow diabetes. That's what they said in the 1800.
Again, not entirely true. We knew about diabetes first in 1500 BC - the difference between Type 1 and Type 2 was not identified until much later (see above). Insulin was discovered in 1921, over 100 years ago, by Frederick Banting and Charles Best. Second, Michael is perpetuating some misinformation here. Here is a great article explaining how “quick and thin diabetes” vs “fat and slow diabetes” was not a distinction between T1D and T2D: The Historical Myth of Thin and Fat Diabetes - Canadian Journal of Diabetes.
As medical science matures, it becomes clear that this is not a good way to talk about these two forms, partly because people are talking at this time about juvenile-onset and mature-onset diabetes.
This isn’t a fact check, but just an interesting point that today, maturity-onset diabetes refers to an entirely separate diagnosis from T1D and T2D.
It's basically just a total jungle around what are we calling these two forms. As early as the 1950s, people just started calling them type 1 and type 2 because we don't know what the fuck we're doing. None of this is working. Let's just say type 1 and type 2 because they don't contain any actual information about who is getting it and when. These terms started coming into use and you can actually look on Google Scholar, which is how I found this. For old papers, they're mostly an international development. People going to Africa and identifying like type 1 and type 2 diabetes cases there. This bounces around in the 1950s.
It’s thought that the first person to use “Type 1” and “Type 2” was John Lister, in 1951. He wrote: there are “two broad groups of diabetics—the young,thin, non-arteriosclerotic group with normal blood pressure and usually an acute onset to the disease, and the older, obese, arteriosclerotic group with hypertension and usually an insidious onset. [...] These types we have provisionally designated type I and type II, respectively.” In other words, these terms were intended as placeholders, because we didn’t know much more. The discussion here, in addition to being factually incorrect, is incredibly problematic. I wonder if Michael has ever read The Emperor of All Maladies, or any other book which details the history of disease discovery and scientific/medical advances. Just because we don’t fully understand something doesn’t mean that we can’t start to notice patterns and categorize things. This is the normal course of medicine - we use the best evidence we have at any time to try to cure or treat disease. It’s frankly offensive to scientists and doctors who were working in this field at the time to act like these people didn’t know what they were doing. It’s also not relevant to harp on them being called Type 1 and Type 2.
Also, I would love to know exactly what Michael searched for in Google Scholar, because I don’t see anything like what he is suggesting in terms of most “old” papers being in international development (side note: what he is describing is not international development, but global health). I’m also unclear what the problem with studying diabetes in Africa is. This seems like a pretty problematic take.
…then in 1976, a researcher named Andrew Cudworth identifies the actual genetic marker of type 1 diabetes.
He's the one that proves that this has a hereditary component. Andrew Cudworth writes a paper basically resurrecting this type 1, type 2 distinction, where he's like, "It really just doesn't make sense to talk about this as juvenile onset and adult onset, when one of them is an autoimmune condition and the other one isn't, and we don't really know what causes it. None of these terms are just very accurate."
Not correct (although this is what Wikipedia says!). Jørn Nerup was actually the first to publish on this in 1974. Cudworth came along after. Also, Cudworth definitely did not say, ‘we shouldn’t refer to it as juvenile onset and adult onset’. In fact, the conclusion of the 1976 paper reads: “In juvenile-onset diabetes or insulin-dependent diabetes irrespective of age of onset there is good evidence that one or more HLA-linked genes are important in producing susceptibility.” He uses both terms.
But then another thing that drives me nuts about the story, this is decades before we have any panic about childhood obesity. Obesity rates don't start rising really in earnest until the 1980s. The panic over childhood obesity is a mid-2000s thing. This is taking place in the mid-1970s. I've attempted to read some of the papers that Andrew Cudworth wrote about this and they're extremely technical. It's like, this receptor on the HB2 tendril or whatever, these are scientists having debates about the nomenclature of something within their field. At no point in any of these papers, just like there's too many fat kids, so we have to rename diabetes comes up. Basically, in 1979, the American Diabetes Association officially recognizes this type 1, type 2 thing and he's like, "Yeah, this is the way forward." And then the WHO recognizes it in 1980. That's how all that happened.
Prior to this point, Michael and Aubrey have not said anything about how calling it juvenile-onset diabetes has anything to do with childhood obesity, so this seems to come out of nowhere. I don’t know what “story” Michael is referring to, but I haven’t seen anything suggesting that is the common belief. That is to say, I’m not sure where this idea came from that people thought it was called juvenile-onset because of fat kids. So it doesn’t seem like this needs to be “debunked.”
This whole thing of like, "Oh, they had to rename it." Not only is it not true, this is in the Wikipedia entry for the history of diabetes. This is not some secret hidden figures, untold history of diabetes. This is extremely mainstream stuff and yet this claim shows up everywhere. It's the same thing with a 90 billion number. It's just like, "I just need a sentence in this man." We all know obesity is really bad and all the kids are dying. So, I just need to throw in something. And you don't even do the most basic fact checking of any of the claims that end up in your article. That's how these zombie statistics run around. Anyway, annoyed.
Again, I’m not sure what this “whole thing” is. Michael and Aubrey haven’t provided any evidence of “this whole thing.” I also think it is a bit ironic for Michael to call out people not doing “the most basic fact checking” because, as you can see, MP has a lot of errors that “the most basic fact checking” could fix.
Okay, hang on. A recent study in the Journal of the American Medical Association predicts that a child born in 2000 has a one in three chance of developing diabetes. An African-American child's chances are two in five… First of all, that's a weird roundabout way of just saying like how many people in America have diabetes?
This is not at all a “weird roundabout way of just saying like how many people in America have diabetes.” In fact, we’ve all definitely seen statistics like this before. It is the standard way that breast cancer risk is presented, in fact (see below). Statistics are often presented like this to make them easier to understand.

The prevalence rate of diabetes in the US, I've seen various estimates. It's somewhere between 7% and 12% of Americans have diabetes.
Epidemiology nitpick: prevalence is not a “rate” - it’s a proportion.
People born now have a one in three chance of getting a disease that only utmost 12% of people have. This comes from a 2003 article called the lifetime risk for diabetes in the United States and it's one of these studies that we've talked about a lot. It's a big old cohort study. They have hundreds of thousands of people, and they ask them the same questions, the same battery of questions every year, and then at the end, they tally what these are the correlations, dah, dah, dah. There's a survey question in this cohort study that says, "Have you ever been told by a doctor other than during pregnancy that you have diabetes or sugar diabetes?" I don't know what the second one is.
Here is the paper that Michael is referencing. It’s a strange choice of study, since it’s so old. The methods section says pretty explicitly what the two questions are: the second one was, “How old were you when a doctor first told you that you had diabetes or sugar diabetes?" The incidence of diabetes is increasing, so the prevalence right now (i.e., the proportion of people with diagnosed diabetes now) is not going to be the same as the predicted prevalence in, say, 20 years. That’s why the 1 in 3 number is different from 12%. Prevalence is just a snapshot in time!
That's weird. They have 356,000 respondents and they get 14,000 yes answers. 4% of their respondents said, yes, I have been diagnosed with diabetes at some point. 4%. And then from this, they do a bunch of statistical mumbo jumbo, and they come up with a 33% chance for men and 39% chance for women of being diagnosed with diabetes at some point in their life. It's a projection of the future. It's being written in 2003 and it's about kids born in 2000. But read the sentence again.
This is a good opportunity to discuss Markov modeling! This is a really great place to start: Markov Chain Tutorial for Toddlers-1 | by Abhishek Khare | Dev Genius. Basically, the authors are creating a model that predicts future occurrences. It’s not as simple as just calculating the prevalence. So, in addition to the “14,325 prevalent cases of diagnosed diabetes among the 356,787 respondents in the NHIS for 1984-2000,” there were, “1349 incident cases of diagnosed diabetes among the 343,856 nondiabetic NHIS respondents for 1984-2000.” The authors can use this, and the different rates by subgroups (age, race/ethnicity, etc.) and include information about how the population is changing, to predict the lifetime probability of being diagnosed with diabetes. Again, this is not the same as prevalence. Very different statistics IF (as in this case), the rates are changing and the population make-up is changing.
It’s not surprising that it’s about kids born in 2000, because it’s using data up until 2000 to predict the future! That’s how predictive models work.
A recent study in the Journal of the American Medical Association predicts that a child born in 2000 has a one in three chance of developing diabetes. Boy, I missed that predicts.. I missed the, we're looking into a scientific crystal ball part.
Again, predictive modeling is very common. We used that during COVID, too! And for cancer! And for basically all diseases! No crystal balls. That’s just how predictive modeling works. 🙂
Michael: Also, when it says, a child born in 2000 has a chance of developing diabetes, don't you think childhood diabetes? …This study is of lifetime risk. One of the findings that stuck out to me in this study is that, the mean age of diagnosis of diabetes is 57 years. In the study it says, "In the cohort of individuals born in 2000, we estimate that 0.88% of males and 1.1% of females will develop diabetes by age 20." So, your chances of getting diabetes by age 20 are around 1%.
Aubrey: Significantly less than the estimated prevalence of eating disorders at those ages.
So this paper does not say anything about “a child born in 2000”. What it DOES say, is “For individuals born in the United States in 2000, we estimate the lifetime risk of diagnosed diabetes mellitus to be roughly 1 in 3 for males and 2 in 5 for females.” In other words, it is VERY clear that it is lifetime risk.
Here is the rest of the sentence that Michael didn’t include: “...by age 40 years, 4.05% and 7.19%; by age 60 years, 18.09% and 20.38%; and by age 80 years, 30.77% and 35.08%, respectively.” This is because most people develop diabetes later in life. I am not sure why Michael is calling this out. It’s also entirely irrelevant what the estimated prevalence of eating disorders at those ages is. It is disturbing that Aubrey is dismissing a very serious health condition simply because there is another health condition that is more prevalent in a certain age group. What is the purpose of this?
Michael: Exactly. By age 40, your chances are somewhere between 4% and 7%. By age 60, your chances are somewhere between 18 and 20%. So, almost all of the risk is coming from people older than 60.
Aubrey: Well, and again, these are framed in a way that's pretty misleading, and again, relies on weight stigma, and panic about fat kids in order to carry the message forward. The message is a deeply stigmatizing one here.
I don’t see what is misleading about this or what is stigmatizing. The words in this article are very measured. Lifetime risk begins in childhood. That’s the nature of estimating lifetime risk.
Michael: Well, that's the thing. If what we're talking about is childhood diabetes, why wouldn't you just list the prevalence of childhood diabetes?
But this paper isn’t about childhood diabetes! It never says it is! It is clearly titled “Lifetime Risk for Diabetes Mellitus in the United States” - no mention of kids!! There isn’t a SINGLE mention of children in the introduction.
Michael: The only reason you would use this weird prediction is because you want a big scary number for people.
Again, no. Where are they getting this from? This article is VERY clear about what it is doing. Michael is twisting it to make it seem like it’s problematic when it absolutely is not.
Michael: There's also the thing that, if what we're really talking about is people over 60 being diagnosed with diabetes, if you're born in 2000 by definition, by the time you're 60, it's 2060. There's also presumably some new treatments and technologies available. So, it's also this weird fear mongering about people being diagnosed in 60 years with diabetes.
This is the “predictive” part! There is no fear mongering happening here. It’s a scientific paper! Treatments and technologies are not the same as preventing the disease. It’s wayyyyy better to prevent a condition than to have to treat it once it occurs.
Michael: A lot of this stuff is just like we're all going to die and it just isn't true.
No one is saying we are all going to die. This is rage baiting.
Michael: Right. But then also, what's so striking to me about this research is that, with all of the scare stories we've read about childhood diabetes and stuff, how much coverage have we actually gotten that engages with those actual kids, and their parents, and their needs? Childhood diabetes, it's a really complex phenomenon.
Where are the scare stories? There is actually a LOT of research on quality of life in this population, it’s just that Michael isn’t looking for it. A quick Google search brought up a ton. Here is a sampling:
Do you know who Dr. William Clish is?... He's considered one of the fathers of bariatric surgery… He was the head or something on the American Board of Pediatrics. He was the past president of the North American Society for Pediatric Gastroenterology and Nutrition, trying to look up on Wikipedia, and most importantly for us, he was the doctor in Supersize Me that counseled Morgan Spurlock.
So I’m not sure where Michael saw that Dr. Klish is one of the fathers of bariatric surgery. He’s actually not even a surgeon. He’s a gastroenterologist. The “father of bariatric surgery” was Edward Mason. Most of the history of bariatric surgery was far before Dr. Klish was around. He was one of three doctors who oversaw Morgan Spurlock’s process (including a general practitioner and a cardiologist).
Michael: In 2002, he gave an interview to the Houston Chronicle. He's talking about childhood obesity. He says, "If we don't get this epidemic in check for the first time in a century, children will be looking forward to a shorter life expectancy than their parents."
It’s really interesting that there are a lot of articles that say that this interview happened, but I can’t find the actual Houston Chronicle article. Anyway, it’s worth noting that the only sources that reference it at this point are those calling it scaremongering, which is totally true and great that it is being called out as such.
Exactly. In 2005, you get a paper in JAMA called a potential decline in life expectancy in the United States in the 21st century that goes through this whole history where it's like, American life expectancy has increased significantly, steadily for the last one hundred years. Infant mortality has fallen, after World War II, we get antibiotics. It used to be roughly a third of Americans were dying of infectious diseases. They get the flu or pneumonia, these things. This is one of the great successes of humanity of the 20th century. Huge deal, steadily increasing life expectancy. But then all this panic about obesity and how obesity is going to be the first generation of kids to die and their parents, whatever, all of this comes from the fact that the rates of growth in life expectancy have started to slow.
This article is actually in NEJM, not JAMA.
Progress is slowing down. This is happening in the late 1990s. They do all of the whole thing again is just empty statistical mumbo jumbo. The whole thing is like, "What would happen if everyone in the country who had an overweight or obese BMI instantly, magically attained a BMI of 24?" That's what they're basing this whole thing on.
Calling it “empty statistical mumbo jumbo” is offensive and anti-science. Michael may not understand the statistics, but that doesn’t mean it is “mumbo jumbo”. It also very explicitly does not say anything about instantly attaining a BMI of 24. It says “if everyone who is currently obese were to lose enough weight to obtain an ‘optimal’ BMI, which we defined as a BMI of 24.” The issue here is not whether or not this is a problematic anti-fat paper. The issue is whether Michael is reporting it correctly, which he is not. It is really important not to dismiss statistical methods just because you don’t understand them. Michael doesn’t know statistics well enough to assess if the statistical methods are appropriate.
Fat people have existed and also exist. This is a sidenote, but it also does this thing, where it just mentions that the BMI doesn't work for black people. It's doing all this like, mortality rates, BMI, and then it's like, "Oh, yeah, anyway, BMI isn't connected the mortality rates for black people. Any black person above 60, it just doesn't really work for them." Anyway, [laughs] I'm just like keep going.
This is absolutely not what the paper does. It says, “When a BMI of 30 or 35 did not lead to lower death rates than the optimal BMI of 24, it was assumed that there was no change in the conditional probability of death. This occurred for black males at 62 to 85 years of age at a BMI of 30 and at 67 to 85 years of age at a BMI of 35, and for black females at 60 to 85 years of age at a BMI of 30 and at 67 to 85 years of age at a BMI of 35.” Contrary to what Michael said, it is not for all Black people, and it isn’t about it “not working.” We have already discussed that BMI is not a good indicator of health or mortality. This is actually the authors acknowledging that this was the case in these subgroups. They didn’t like “keep going.” This is another problematic misrepresentation of a scientific study.
This isn't even the original claim that was made. The original claim that was made was that this generation of children, people born now are going to have shorter life expectancies than their parents. That's not what this is showing. It's showing that rates are going to continue to increase, but they would have increased more if it wasn't for obesity.
I’m not sure why Michael thinks that this paper has anything to do with Dr. Klish’s claim, as it doesn’t cite him anywhere, nor does it state the “original claim” anywhere. This is not supposed to be a direct response to that.
But why would we assume that current rates of death associated with obesity would remain constant? Deaths associated with obesity have fallen precipitously.
First, this is incorrect. Second, this is a good opportunity to take a step back and look at a common issue with MP. If you recall, in the episode, “Is Being Fat Bad For You?” Michael and Aubrey effectively say that you can’t possibly attribute death to obesity, because what you’re actually doing is attributing death from another cause in an obese person to death due to obesity. Now, however, Michael is changing his tune and using that exact same statistic that he previously disagreed with in an attempt to support his argument. Unfortunately, he doesn’t provide any citations, and all of the evidence suggests that, if, in fact, we do attribute deaths among obese individuals to obesity, those deaths are increasing.
You are significantly less likely to die of a heart attack now than you were in 1950. Even cancer, I found a really interesting analysis of this, like, changing mortality statistics in America. Since 2011, since very recently, cancer death rates are down 20%, heart disease death rates are down 10%.
These points are irrelevant. The statement is about deaths due to obesity, not heart attacks or cancer.
Yeah, and also, again these are all presumed to be causes of death that are related to being fat. And that also hasn't been fucking established.
No, these are not presumed to be due to being fat. These are separate. Please return to the episode “Is Being Fat Bad For You” and look at the papers there.
Right. It drives me nuts. It is the same researcher who wrote this paper being like, "Oh, we're all going to die. Life expectancy getting shorter." He writes another paper in 2009 that is completely unrelated to this. It's Social Security Administration projections. A million institutions project US life expectancy for various things, where he predicts that the Social Security Administration and the CDC's life expectancy predictions are not optimistic enough. He says life expectancy for Americans is going to keep increasing and it's probably going to be 87 years by 2050.
The paper was quite a bit more complex than Michael suggests. I don’t know where Michael got the 87 from, because there are a lot of numbers being thrown around in this paper and 87 isn’t one of them. The actual results say, “If death rates are reduced by 2050 because of continued and accelerated gains made against major fatal diseases (scenario A), life expectancy at birth [e(0)] would rise to 83.2 for males and 89.2 for females by 2050 (see table 2). These forecasts are 3.6 percent higher than the Census Bureau's forecasts and 5.2 percent higher than the SSA's forecasts. If death rates were reduced by 2050 by efforts to slow aging (scenario B), then e(0) would rise to 85.9 and 93.3 for males and females, respectively, (table 2), figures that are 7.3 percent higher than the Census Bureau's and 8.8 percent higher than the SSA's. The Social Security Administration's middle-range forecasts indicate that in 2050 e(0) will be 80.0 and 83.4 years for males and females, respectively (table 2). The Census Bureau (CB) forecasts that in 2050 e(0) for males and females will be 80.9 and 85.3 years, respectively.”
Oh, so, when you're not writing about obesity, you're going to be like, "Oh, well, actually, this is what the data indicates. But I had to write an article that was scaring people about obesity. I did some weird statistical show with that." You find this all over the place. You find this with some of the economic analyses, too, that when they're writing for an obesity audience or for a Public Health Journal, that would be like, "Obesity is the biggest killer." And then you'll find the same author with a paper that has something to do with something completely else and they're like, "Oh, yeah, obesity is really not that big of a deal."
I’m not defending this paper, but it is absolutely not an about-face. They explicitly stated “For example, if recent trends in childhood and adult-onset obesity are not reversed in the United States, it is possible that the life expectancy of some subgroups of the population could fall within the next few decades (Olshansky et al. 2005). The forecasts presented here do not repudiate that line of reasoning.” (emphasis mine) This guy is not going back on his prior work, despite what Michael says (and despite the fact that his prior work was problematic).
Michael: Exactly. They want to raise the alarm about obesity. It's like, "Oh, it's a public health problem. We have to do something about it." But you're not really being transparent about the fact that that's what you're doing. The same author, he admits in this paper, he's like, "Oh, yeah, I wrote another paper a couple years ago saying that obesity might shorten lifespan, but that was only if we do nothing. My actual projections for life expectancy in 2050, I'm just assuming that the reductions in the death rates are going to continue. I didn't do that in that previous paper."
Again, see the quote above. That’s quite clearly NOT what the paper says. It very clearly holds the line about obesity and life expectancy. There is absolutely nowhere in this paper that he says anything like what Michael says here.
This is what really bugs me about this is that, you expect the Michael Pollan's of the world journalists to do this kind of thing, whenever. I'm trying to raise awareness, I need this paragraph in my story being like, "Here's a bunch of scary statistics about obesity." Whatever. We expect that from journalists. But what we see here is, there's a pipeline of academic institutions that are producing numbers for exactly this purpose. They are producing numbers, so that it can show up in the Surgeon General's report, it can show up in media reports, it can go on the CDC website, whatever to raise awareness of this, what they perceive to be a public health problem. I think on some level, I get it. If you're a smoking tobacco researcher, if you're a climate change researcher, I get that you want to get science out there in a way that is going to inspire people to take action.
There is no “pipeline of academic institutions that are producing numbers for exactly this purpose.” That is a dangerously anti-science and reductionist view. There are tons of academics who disagree with Olshansky - you can find debates about this with a quick Google search. James Vaupel, specifically, was an academic who strongly disagreed with Olshansky. This is not a systemic “academia” problem. Also, this is a bit of the pot calling the kettle black, given that Michael and Aubrey do a lot of picking the numbers they want.
But the problem is, I think that this has gotten away from people, that they've forgotten how many assumptions they're making, they've forgotten how thin this correlation stuff is, and they've forgotten that the purpose of all of this. If all of this raising awareness, all of this is supposed to be for public health, it's supposed to make people healthier. What we see again and again in these studies and the way that these studies are covered in the media is that, we're giving up on public health, so, we can warn people about obesity.
Michael and Aubrey really like to talk about correlation, but they actually don’t understand what “correlation” really is. To be clear, “correlation” is relevant only in linear relationships. In fact, statistical dependence (i.e., statistical significance) can exist even in the absence of correlation, if variables are related in a non-linear way. So sure, correlation does not equal causation, but causation also does not equal correlation.
Right. I also think it allows public health institutions to find one of the few things for which there is a case for personal responsibility or something that they see as an individual change, something that they can do something about. What I found in a lot of the research that I read for this was public health having an existential crisis over the last 40 years, a lot of our public health institutions are set up for communicable diseases. They're set up for things like, "Okay, there's a Legionnaires disease outbreak at some hotel in Michigan and we got to fly a bunch of people out there, we got to isolate, we got to do contact tracing, we got to figure this out, tamp it down." Something acute… Whereas public health institutions, when it comes to non-communicable diseases, a lot of these institutions are really flailing, because there isn't a lot that they have in their power to do. A lot of this stuff comes down to weird, esoteric shit, like, urban policy, and housing policy, and welfare, tax policy, and all kinds of other stuff. Because a lot of these diseases are actually diseases of inequality. As you said last episode, this gets very political very fast and I don't think that Institutions of Public Health and institutions of science and medicine, they're not set up to do these more holistic analyses of problems.
I don’t know how Michael could possibly have assessed this from the research. As someone with an actual degree in public health, I can tell you that communicable diseases are the bottom of the totem pole. They get very little funding and attention. If all of our systems had been set up for communicable diseases, COVID would not have had such an enormous impact. I also don’t know exactly which “institutions” Michael is referring to here. Public health is not a monolith. Does he mean government institutions? Academic institutions? Hospitals? Very unclear. Most importantly, communicable diseases are ALSO diseases of inequality. We have a huge inequity issue in our medical system.
It’s also pretty offensive (and patently false) to say that “institutions” aren’t “set up to do these more holistic analyses of problems.” There are thousands of researchers looking into social determinants of health. If you take a look through any of the literature, you will see some really fantastic studies in this space. The problem is not the analyses, it’s developing and implementing solutions. It’s just wrong to say that we need more analysis of these things - what we need is to find ways to fix things.
Yeah, it's so frustrating, because we get so attached to having these cultural conversations about health in a vacuum as if they are somehow uninfluenced by social, or political, or institutional dynamics. And actually, what the research shows and what the lived experience of marginalized people shows is that, our understandings of health are a direct result of those institutional, and cultural, and political factors that it is a pretty straight line between what our institutions decide to do and the health outcomes of any given population. It's frustrating to have so many conversations about this kind of stuff that are like, "No, no, no, I just want to talk about the science." It's like, "Buddy, you can't talk about the science without talking about the bias that is baked into the science. Sorry."
Again, if you read the scientific literature, you will see that there is a TON of research looking at the influence of sociopolitical and institutional dynamics. It’s a huge area of epidemiology research, specifically. The way that Aubrey and Michael portray the research makes it seem like these things happen in a vacuum, but that’s because they are misrepresenting the studies.
Thank you for reading, if you got this far!
Heya - found you through a Reddit comment and just wanted to drop a note of appreciation/encouragement. Coming from the policy side of things, am similarly puzzled and fairly alarmed by the runaway popularity of Maintenance Phase, so really appreciate your thorough deconstruction of the fluffy, “feel good” narratives pumped out by the pod.
Have you ever considered recording a version of your critiques a la Decoding the Gurus?
Thank you for this! I’ve also listened to some Hobbes episodes (particularly “if books could kill”) and done some of my own fact checking -- he has a very bad tendency to grossly misrepresent studies or leave out important context that would be impossible to miss to anyone with even average familiarity with particular topics.
When he started talking about things related to my own PhD work I couldn’t help but notice approx. 1 billion mistakes in interpretation and representation. This was doubly frustrating because his takes were conveyed with extreme smugness 😅